Position statement
Prevention and management of neonatal herpes simplex virus infections

Posted: Mar 6, 2020 | Updated: Oct 10, 2025 | Reaffirmed: Jan 12, 2026
Principal author(s)
Upton D Allen, Joan L Robinson; Ari Bitnun; Jane McDonald; Canadian Paediatric Society, Infectious Diseases and Immunization Committee
Abstract
Human herpes simplex virus (HSV) infection in neonates can result in devastating outcomes, including mortality and significant morbidity. All infants are potentially at risk for neonatal HSV infection. This position statement reviews epidemiology, transmission and risk factors, with a focus on intrapartum infection. It considers diagnosis and prognosis according to infection category, along with testing modalities and limitations. Recommendations for managing newborns known to have been exposed intrapartum to HSV are based on expert opinion because a randomized trial to compare management options is not feasible. Guidance is provided for the empirical management of infants with suspected clinical sepsis, including those who do not respond to antibacterial therapy. The present statement replaces a 2006 position statement by the Canadian Paediatric Society.
Key Words: Acyclovir; CNS; Encephalitis; SEM; Sepsis
Epidemiology
Estimated rates of neonatal human herpes simplex virus (NHSV) infection vary across different regions of the world.[1][2] In Canada, the infection occurs in approximately one per 16,500 newborns, which corresponds to approximately six per 100,000 live births.[1] Transmission to newborns can occur with either genital herpes simplex virus (HSV) type 1 (HSV-1) or HSV type 2 (HSV-2). Worldwide, an estimated 75% of NHSV cases are caused by HSV-2 and 25% by HSV-1.[3] One Canadian prospective study analyzing reports in the period between 2000 and 2003 found that 63% of cases were due to HSV-1.[1] Studies from Ontario (conducted in 2000 to 2001)[4] and British Columbia (in 1999)[5] investigating infants potentially at risk for HSV-2 detected HSV-2 antibodies in 10% and 17% of pregnant women, respectively.
Many factors influence the transmission of HSV infection to newborns, including the nature of maternal infection, the mode of delivery, the duration of rupture of membranes and the use of intrapartum instrumentation.
Maternal genital HSV cases may be classified as follows:[6]
- Newly acquired
- First-episode primary infection (mother has no serum antibodies to HSV-1 or -2 at onset);
- First-episode nonprimary infection (mother has a new infection with one HSV type in the presence of antibodies to the other type); or
- Recurrent (mother has pre-existing antibodies to the HSV type that is isolated from the genital tract).
The most common and important category of NHSV acquisition is intrapartum. Even for HSV-1, >75% of cases of NHSV are acquired during delivery from genital disease that is often newly acquired and asymptomatic.[7] Newborns may also acquire HSV infection through in utero or postnatal transmission. Although rare, in utero HSV infection can have teratogenic effects such as skin lesions or scars, central nervous system (CNS) disorders and chorioretinitis.[8] Postnatal infection can be acquired from the infant’s mother or from nonmaternal sources (eg, relatives or hospital personnel with orolabial herpes or asymptomatic shedding of HSV-1).[3][9]
In most cases of NHSV infection, there is no known history of maternal genital HSV because mothers have never had or have never noticed external genital lesions. Studies show that 75% to 90% of individuals who are seropositive for HSV-2 were unaware of their infection.[10] All infants, therefore, must be considered to be potentially at risk for NHSV infection. Seropositive women intermittently shed HSV in their genital tracts, with 10% to 20% of individuals with HSV-2 shedding on any given day, as detected by polymerase chain reaction (PCR) testing.[11]
The category of maternal infection at time of delivery influences the likelihood of NHSV acquisition, presumably because mothers who have had an HSV infection transmit HSV-neutralizing antibodies to their infant across the placenta, provided that their infant is not born before 32 weeks’ gestation.[7][12]-[14] Thus, infants born to mothers who have a first-episode primary infection at time of delivery are at the highest risk for acquiring HSV, with transmission rates of up to 60%, because their mother had no pre-existing neutralizing antibodies to transmit.[3] For infants born to mothers who have first-episode nonprimary infections, the transmission rates are in the order of ≤30% because crossreactive antibodies are present. The lowest risk of neonatal transmission occurs with maternal recurrent infection (at <2%) because type-specific antibodies are present.[4]
Delivery by elective Cesarean section markedly reduces but does not eliminate the risk for newborn infection.[15][16] Women with recurrent genital HSV are commonly prophylaxed with acyclovir (ACV) or valacyclovir from 36 weeks’ gestation until delivery. In this context, antiviral therapy near the end of pregnancy can lower recurrence of genital HSV and shedding at delivery;[17] however, it is not clear whether this prophylaxis translates to a reduced risk for NHSV infection. Guidelines regarding the role of Cesarean delivery and the indications for acyclovir are published[16][18][19] but are not specifically addressed in the present statement.
Obstetrical procedures that can cause scalp abrasions or a break in the infant’s skin during labour and delivery may increase risk of NHSV transmission to a newborn infant. Fetal scalp sampling and monitoring, use of forceps and vacuum-assisted deliveries[16][19]-[23] should be avoided if possible when maternal genital lesions are present.[16] Early or prolonged rupture of membranes may also increase risk.
Categories and outcomes of NHSV infection
Classifying NHSV infections can help to guide diagnosis and management, and is important for assigning prognosis.[24] Intrauterine NHSV infections are rare, accounting for <5% of cases. The classification of infection acquired in the perinatal, natal and postnatal periods is as follows:
- Disseminated HSV;
- Localized CNS HSV;
- Skin, eye and mucous membrane (SEM) infection.
There may be overlap among the different syndromes. Disseminated disease involves multiple organs, notably the liver and lungs.
In most cases, the initial symptoms of NHSV infection present within the first four weeks of life. Occasionally, disease presents for the first time between four and six weeks after birth;[4] therefore, infants up to 42 days of age should be fully evaluated for NHSV when clinical features are consistent with NHSV. Newborns with intrauterine infection present at birth or shortly thereafter.
The absence of skin lesions does not negate the possibility of an NHSV diagnosis. One study showed that 39% of infants with disseminated disease did not have skin lesions at any time during their illness, while 32% with CNS disease and 17% with SEM disease did not develop skin lesions.[25] NHSV infection should be considered in neonates with sepsis syndrome, particularly when this condition is accompanied by liver dysfunction and even when there is no known history of maternal HSV and the infant has no skin vesicles. One study reviewed 32 infants with perinatal HSV, noting that 50% of cases came to medical attention with nonspecific complaints and 75% of these had fever alone. Nonspecific presentation occurred primarily in infants whose symptoms started at <21 days of age.[26] Also, HSV should be considered in neonates with fever, irritability and abnormal cerebrospinal fluid (CSF) findings, particularly when accompanied by seizures. However, a normal initial CSF examination does not necessarily exclude the diagnosis of an NHSV CNS infection.[26]
Infants who present with disseminated disease are less likely to survive than infants with SEM or CNS disease. Data suggest that dissemination is more common with newly acquired maternal HSV, presumably because there has not been sufficient time to transfer neutralizing antibodies in utero.[27][28] Before antivirals, an estimated 85% of infants with disseminated HSV disease and 50% with CNS disease died.[29] Treatment with ACV (60 mg/kg/day) has resulted in one-year mortality rates from disseminated and CNS disease of 29% and 14%, respectively.[30] A mortality rate of 15.5% was reported in a Canadian study that documented cases occurring over a three-year period (October 2000 to September 2003).[1]
Among survivors enrolled in two studies of parenteral ACV for which follow-up data were available at 12 months of age, 25% of patients with disseminated disease exhibited neurological complications, compared with 70% with CNS infection alone.[25] Among neonates with SEM disease (without apparent CNS disease), long-term neurological sequelae have also been documented.[28][31] However, more recent studies demonstrate no sequelae; therefore, it appears likely that those infants with sequelae had unrecognized CNS infection.[32]
Laboratory diagnosis
It is important for the clinician to speak with a laboratory specialist or infectious disease consultant when NHSV is suspected, particularly in settings where testing for NHSV is performed less frequently. Expert consultation is important because the utility of testing modalities varies according to sample type, and the laboratory must provide general as well as centre-specific advice on the types of specimens to send for testing. Each specific laboratory test for HSV has important limitations. Therefore, test results should be interpreted with careful consideration of the clinical context and results from nonspecific investigations including an electroencephalogram, computed tomography or magnetic resonance imaging, liver transaminase levels and platelet count.
HSV may be detected by viral culture, direct immunofluorescent antibody staining or enzyme immunoassays. However, PCR testing of CSF, skin lesions, mucous membranes and blood is thought to be more sensitive and is now offered by most laboratories.
The detection of the virus in superficial cultures may represent skin contamination by intrapartum exposure if samples are obtained within the first 24 h after birth.[4] When samples obtained >24 h after birth are positive, they are more likely to represent active viral replication than contamination. Prospective studies regarding the utility of periodic surveillance cultures in the early diagnosis of NHSV infection are lacking for infants exposed to active genital lesions.
Caution should be exercised when using a negative CSF HSV PCR to rule out CNS HSV, particularly when the sample is obtained in the early stages of illness (the first 24 h to 48 h). If the index of suspicion is high, yet the CSF PCR is negative, there are two options that could be considered. A repeat CSF PCR within 72 hours of starting acyclovir is likely to be positive in infants with CNS HSV. Alternatively, one could complete 21 days of IV acyclovir for possible CNS HSV. Because CNS disease can be very subtle, any patient with suspected NHSV infection should have a lumbar puncture performed for CSF HSV PCR testing as soon as it is clinically feasible to do so, unless there is a contraindication to performing a lumbar puncture. CNS NHSV infection may occur despite ‘normal’ CSF cell counts and biochemical features, particularly in the early stages of infection. Therefore, the CSF HSV PCR test should be performed even when these parameters are normal.
The evaluation of HSV viremia using PCR is less well established than CSF PCR testing. [33]-[35] One study that evaluated HSV viral load in serum and CSF using a real-time PCR assay found that patients with disseminated disease had higher viral loads in their sera, while patients with CNS infection had higher viral loads in their CSF.[33] Viral loads were also higher in patients who succumbed to HSV disease, suggesting that this measure may be useful for assessing prognosis in NHSV cases. A poorer prognosis has also been associated with persistence of HSV in the CSF of patients on acyclovir.[33]
There is limited experience with PCR testing of respiratory specimens but a positive result from a nasopharyngeal specimen of an infant with pneumonia makes it highly likely that the infant has disseminated NHSV infection.
Infant serology is not useful for diagnosing NHSV for three main reasons. First, transplacental immunoglobulin (Ig) G antibodies cannot be differentiated from IgG produced by the infant. Second, the ability of some severely affected infants to make antibodies is impaired. Third, the commercially available assays for HSV IgM antibodies have only variable and limited reliability.
Managing NHSV infections
Intravenous acyclovir is the treatment of choice for treating NHSV. The dose is 60 mg/kg/day in three divided doses administered every 8 h, assuming that renal function is normal.[30] The duration of therapy is dictated by the category of disease. For SEM disease, the duration of therapy is 14 days, while for disseminated or CNS disease, the minimum duration of treatment is 21 days. Oral ACV has limited bioavailability, resulting in inadequate drug levels for treatment;[36] consequently, parenteral therapy is required. The use of higher doses of ACV is associated with neutropenia and adequate hydration is necessary to reduce the risk of nephrotoxicity.[30] A topical agent (eg, 1% trifluridine) is recommended for use with parenteral ACV in neonates with ocular disease.[3]
Given the potential for significant neurological sequelae in survivors of NHSV infection, affected infants should have a structured follow-up program that allows for neurodevelopmental, ophthalmological and hearing assessments.
There has been research into the role of suppressive antiviral therapy in infants with NHSV infections. A randomized, double-blinded, placebo-controlled trial evaluated infants with CNS HSV or disseminated HSV with CNS involvement, while a second, parallel trial evaluated infants with SEM HSV disease. The study demonstrated improved developmental outcome in infants with CNS involvement who were randomly assigned to receive six months of treatment with oral ACV versus placebo.[32] For infants with SEM disease, the only benefit was a decreased incidence of skin recurrences but this can prevent the need for a lumbar puncture and readmission for repeat intravenous ACV with recurrences before 6 weeks of age.[37][38]
Recommendations
Laboratory diagnostics for NHSV infections
- Whenever a diagnosis of NHSV is being considered, it is essential to order laboratory testing for HSV in addition to performing skin and mucous membrane examinations:
- The standard tests for HSV include CSF PCR and swabs of vesicular lesions and mucous membranes. Also, blood for HSV PCR may be tested if disseminated NHSV is suspected. Following discussion with the laboratory, a nasopharygeal specimen should be tested when the infant has pneumonia. Serum hepatic transaminase levels should be measured to provide supporting evidence for disseminated HSV infection.
- When evaluating NHSV infection in exposed asymptomatic infants, mucous membrane swabs should be obtained from the mouth, nasopharynx and conjunctivae at least 24 h after delivery. Additional swabs may be obtained (eg, from sites of scalp electrodes, if present).
- PCR testing for CSF HSV DNA is the diagnostic method of choice for CNS HSV.
- For all the above tests, clinicians and laboratory staff should work together to minimize the turn-around time for test results.
Managing asymptomatic term infants whose mothers have active lesions at delivery (Figures 1 and 2)
- First clinical episode of genital herpes infection, infant delivered by Caesarean section before rupture of membranes
The risk for NHSV is very low. Assuming that the infant is well, mother and child can be discharged pending results of the mucous membrane and nasopharyngeal swabs taken at 24 h of life. Reliable caregivers should be made aware of the signs of NHSV infection. Some experts also recommend testing blood with PCR, if the test is available. If HSV is detected on a swab or in blood PCR, the infant should be managed as a case of NHSV.
Note: With respect to the above, some experts recommend performing CSF cell count, chemistries and PCR when mucous membrane swabs are taken (ie, a complete work-up).
- First clinical episode of genital herpes infection, infant delivered vaginally or by Caesarean section after rupture of membranes
An infant’s mucous membrane swabs should be obtained and ACV started. It remains controversial whether this testing should be performed at birth (with the risk being detection of surface contamination) or at 24 h of life. Some experts also recommend testing blood with PCR, if the test is available. If the infant’s swabs or blood PCR are positive, CSF PCR must be obtained to determine the duration of ACV therapy. If the infant’s swabs are negative, the infant should receive ACV for 10 days despite negative swabs.
Note: Some experts recommend performing CSF cell count, chemistries and PCR when mucous membrane swabs are taken (ie, a complete work-up).
- Recurrent HSV at delivery–Infant delivered by Caesarean section
Use the same approach as for first-episode infections before membrane rupture.
- Recurrent HSV at delivery–Infant delivered vaginally
Obtain mucous membrane swabs at 24 h and the infant may be discharged pending results. Some experts also recommend testing blood for PCR, if the test is available. ACV therapy would only be indicated when the swabs or blood PCR are positive or when the infant develops signs and symptoms of NHSV infection.
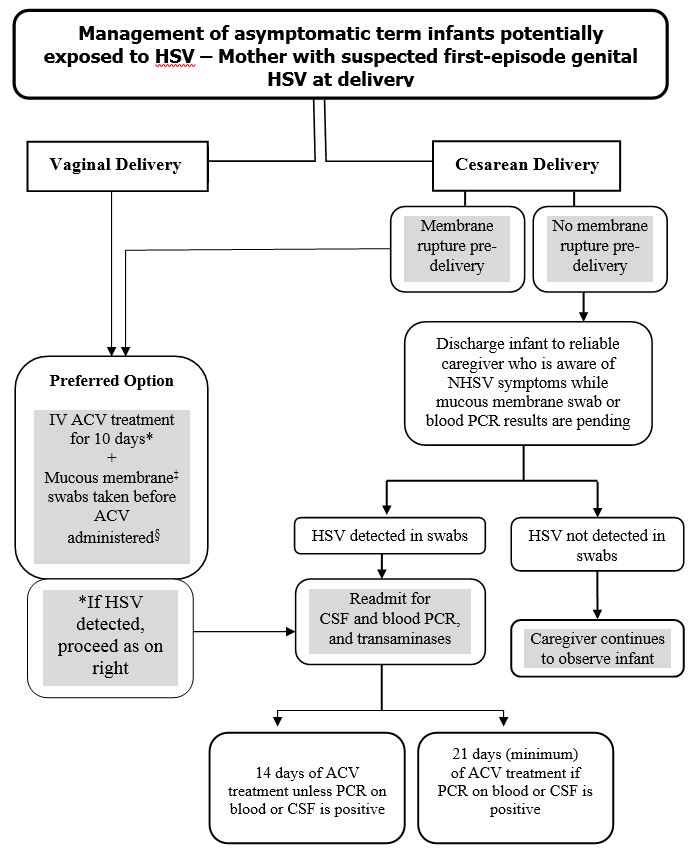 |
| Figure 1) ‡The term ‘mucous membrane swabs’ denotes swabs taken from conjunctivae, mouth and nasopharynx; additional swabs may be obtained (eg, from sites of scalp electrodes, if present). In addition to mucous membrane swabs, some experts recommend blood for polymerase chain reaction (PCR), if this test is available. Clinicians should speak with a laboratory specialist or infectious diseases consultant when neonatal HSV (NHSV) is suspected and laboratory tests are being requested. §Also note that some experts recommend obtaining cerebrospinal fluid (CSF) cell count, chemistries and PCR when mucous membrane swabs are taken (ie, a complete work-up). IV Intravenous |
 |
|
Figure 2) *Some experts consider swabs to be optional if a Caesarean section was performed with no rupture of membranes before delivery. The term ‘mucous membrane swabs’ denotes swabs taken from conjunctivae, mouth and nasopharynx; additional swabs may be obtained (eg, from sites of scalp electrodes, if present).†Assumes observation is performed at home by parents, with or without nursing visits. Clinicians should speak with a laboratory specialist or infectious diseases consultant when neonatal herpes simplex virus (NHSV) is suspected and laboratory tests are being requested. ACV Acyclovir; CSF Cerebrospinal fluid; PCR Polymerase chain reaction |
Managing asymptomatic term infants whose mothers have no active lesions at delivery (including women on ACV prophylaxis)
An infant whose mother has a history of HSV but no active lesions at delivery should be observed for signs of NHSV but does not require ACV therapy. Mucous membrane swabs are not routinely recommended for this infant. In scenarios in which the first clinical evidence of HSV was documented during the third trimester or near delivery, clinicians may consider mucous membrane swabs. Parents and caregivers should be educated about the signs and symptoms of NHSV.
Managing the neonate with symptoms compatible with NHSV
Disseminated HSV can mimic bacterial sepsis, and clinicians need to consider possible NHSV infection in unwell infants <6 weeks of age. Pending laboratory confirmation, consider investigations and treatment of NHSV for the following at-risk patients:
- Infants started on IV antibiotics for suspected sepsis (especially infants presenting with seizure or yielding abnormal CSF) who do not improve rapidly and have negative bacterial cultures at 24 h incubation.
- Infants admitted with pneumonia of uncertain etiology who do not improve after 24 h on antibiotics, especially if the radiographic picture is consistent with viral pneumonia.
- Infants with unexplained bleeding from venipuncture sites or an unexplained, documented coagulopathy.
- Infants started on IV antibiotics for suspected sepsis who are found to have unexplained hepatitis.
Treatment and follow-up of infants with NHSV infections
- Early therapy with intravenous (IV) ACV improves the prognosis for all three presentations of NHSV. Therefore, infants should be started on IV ACV before laboratory confirmation of NHSV, as soon as the infection is suspected clinically.
- The dose is 60 mg/kg/day in three divided doses administered every 8 h, assuming that renal function is normal. Treatment duration should be 14 days if the disease is limited to the skin, eyes or mouth, and a minimum of 21 days if the infection involves the CNS or is disseminated.
- For infants with CNS disease, CSF should be sampled near the end of a 21-day course of therapy. If the PCR remains positive, treatment should be extended with weekly CSF sampling and ACV stopped when a negative result is obtained.
- In combination with parenteral ACV, neonates with ocular involvement should initially receive a topical ophthalmic agent such as trifluridine. An ophthalmology consultation is essential. This may inform the decision to use combination therapy versus monotherapy depending on disease severity.
- Oral ACV is contraindicated for the acute treatment of NHSV because drugs levels are too low. Levels from oral ACV are only high enough for suppressive therapy.
- Suppressive therapy with oral ACV (300 mg/m2 per dose administered three times per day) should be given for six months to infants with CNS disease. A tool for calculating body surface area can be found at: www.csgnetwork.com/bsacalc.html. Data are less convincing for SEM or disseminated disease, but suppressive therapy may still be offered.
- Follow-up is necessary to detect and manage adverse effects related to suppressive ACV treatment as well as for the neurodevelopmental sequelae of NHSV. Complete blood count, and urea and creatinine levels should be checked monthly for adverse effects, and the dose of ACV adjusted for growth. Infants should be followed in a program that enables their evaluation for the neurodevelopmental, ophthalmological and aural consequences of NHSV infection.
Preventing NHSV infections
Strategies to prevent NHSV, including the identification of high-risk pregnancies, Caesarean delivery, maternal antiviral therapy, and anticipatory guidance for prospective mothers and partners, are largely beyond the scope of this statement. However, the following recommendations are especially pertinent to special care nurseries and neonatal intensive care units.
General infection control measures
Comprehensive infection control guidelines are available,[39] but three specific target groups warrant attention here:
Neonates with HSV infection and exposed neonates
- Neonates with HSV infection should be managed using contact precautions when mucocutaneous lesions are present and until lesions have crusted.
- Asymptomatic neonates whose mothers have active HSV lesions should be managed using contact precautions until the end of the incubation period (day 14) or until samples from the infant taken after the first 24 h of life are negative. Some experts do not recommend contact precautions if an exposed infant is born by Caesarean section and membranes are ruptured <4 h to 6 h.
Mothers and other close family contacts with active HSV
- Mothers who are in hospital should be on contact precautions until their lesions have crusted.
- Mothers with herpes labialis should wear a disposable mask when caring for their infant <6 weeks of age until all lesions are healed (crusted and dried). Other close family contacts with herpes labialis should avoid direct contact with the infant or wear a disposable mask if caring for the infant. Advise mothers and other affected family members not to kiss the infant. There is no contraindication to breastfeeding unless there are herpetic lesions on the breast.
- Mothers with skin lesions should keep them covered whenever their newborn is present.
Staff with orofacial or skin lesions
- Staff with skin lesions due to HSV must practice meticulous hand hygiene. Individuals who have contact with infants should keep their lesions covered. If this is not possible, direct care of neonates should be avoided.
- Some experts recommend wearing a surgical mask to cover orolabial lesions because these cannot be covered by dressings.
- Staff with active herpetic whitlow should avoid contact with neonates.
Acknowledgements
This position statement has been reviewed by the Fetus and Newborn and Community Paediatrics Committees of the Canadian Paediatric Society.
CPS INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE
Members: Robert Bortolussi (past Chair); Natalie A Bridger MD; Jane C Finlay MD (past member); Susanna Martin MD (Board Representative); Jane C McDonald MD; Heather Onyett MD; Joan L Robinson MD (Chair); Marina I Salvadori MD (past member); Otto G Vanderkooi MD
Consultant: Noni E MacDonald MD
Liaisons: Upton D Allen MBBS, Canadian Pediatric AIDS Research Group; Michael Brady MD, Committee on Infectious Diseases, American Academy of Pediatrics; Janet Dollin MD, College of Family Physicians of Canada; Charles PS Hui MD, Committee to Advise on Tropical Medicine and Travel (CATMAT), Public Health Agency of Canada; Nicole Le Saux MD, Immunization Monitoring Program, ACTive (IMPACT); Dorothy L Moore MD, National Advisory Committee on Immunization (NACI); John S Spika MD, Public Health Agency of Canada
Principal authors: Upton D Allen MBBS; Joan L Robinson MD; Ari Bitnun MD; Jane McDonald MD
Updated by: Ari Bitnun MD
References
- Kropp RY, Wong T, Cormier L, et al. Neonatal herpes simplex virus infections in Canada: Results of a 3-year national prospective study. Pediatrics 2006(6);117:1955-62.
- Brown ZA, Wald A, Morrow RA, Selke S, Zeh J, Corey L. Effect of serologic status and Cesarean delivery on transmission rates of herpes simplex virus from mother to infant. JAMA 2003;289(2):203-9.
- American Academy of Pediatrics. Herpes simplex virus. In: Kimberlin DW, Banerjee R, Barnett ED, Lynfield L, Sawyer MH, eds. Red Book: 2024 Report of the Committee on Infections Diseases, 33rd edn. Itaska, IL: AAP, 2024:467-78.
- Howard M, Sellors JW, Jang D, et al. Regional distribution of antibodies to herpes simplex virus type 1 (HSV-1) and HSV-2 in men and women in Ontario, Canada. J Clin Microbiol 2003;41(1):84-9.
- Patrick DM, Dawar M, Cook DA, Krajden M, Ng HC, Rekart ML. Antenatal seroprevalence of herpes simplex virus type 2 (HSV-2) in Canadian women: HSV-2 prevalence increases throughout the reproductive years. Sex Transm Dis 2001;28(7):424-8.
- Arvin AM, Whitley RJ. Herpes simplex virus infections. In: Remington JS, Klein JO, eds. Infectious Diseases of the Fetus and Newborn. 7th edn. Philadelphia: WB Saunders, 2006.
- Corey L, Wald A. Maternal and neonatal herpes simplex virus infections. N Engl J Med 2009;361(14):1376-85.
- Marquez L, Levy ML, Munoz FM, Palazzi DL. A report of three cases and review of intrauterine herpes simplex virus infection. Pediatr Infect Dis J 2011;30(2):153-7.
- Kimberlin DW. Neonatal herpes simplex infection. Clin Microbiol Rev 2004;17(1):1-13.
- Gardella C, Brown Z. Prevention of neonatal herpes. BJOG 2011;118(2):187-92.
- Tronstein E, Johnston C, Huang ML, et al. Genital shedding of herpes simplex virus among symptomatic and asymptomatic persons with HSV-2 infection. JAMA 2011;305(14):1441-9.
- Yeager AS, Arvin AM, Urbani LJ, Kemp JA. Relationship of antibody to outcome in neonatal herpes simplex virus infections. Infect Immun 1980;29(2):532-8.
- Brown ZA, Selke S, Zeh J, et al. The acquisition of herpes simplex virus during pregnancy. N Engl J Med 1997;337(8):509-15.
- Sullender WM, Miller JL, Yasukowa LL, et al. Humoral and cell-mediated immunity in neonates with herpes simplex virus infection. J Infect Dis 1987;155(1):28-37.
- Tita AT. When is primary cesarean appropriate: Maternal and obstetrical indications. Semin Perinatol 2012;36(5):324-7.
- ACOG Committee on Practice Bulletins. Clinical management guidelines for obstetrician-gynecologists: No. 82, June 2007: Management of herpes in pregnancy. Obstet Gynecol 2007;109(6):1489-98.
- Hollier LM, Wendel GD. Third trimester antiviral prophylaxis for preventing maternal genital herpes simplex virus (HSV) recurrences and neonatal infection. Cochrane Database Syst Rev 2008;(1):CD004946.
- Money D, Steben M, Wong T, et al. Guidelines for the management of herpes simplex virus in pregnancy. J Obstet Gynaecol Can 2008;30(6):514-26.
- Royal College of Obstetricians and Gynaecologists. Genital herpes in pregnancy, Management (Green-top 30), 2nd edn. 2007: www.rcog.org.uk/files/rcog-corp/uploadedfiles/GT30GenitalHerpes2007.pdf (Accessed January 16, 2014).
- Nahmias AJ, Josey WE, Naib ZM, Freeman MG, Fernandez RJ, Wheeler JH. Perinatal risk associated with maternal genital herpes simplex virus infection. Am J Obstet Gynecol 1971;110(6):825-37.
- Parvey LS, Ch’ien LT. Neonatal herpes simplex virus infection introduced by fetal-monitor scalp electrodes. Pediatrics 1980;65(6):1150-3.
- Kaye EM, Dooling EC. Neonatal herpes simplex meningoencephalitis associated with fetal monitor scalp electrodes. Neurology 1981;31(8):1045-7.
- Kohelet D, Katz N, Sadan O, Somekh E. Herpes simplex virus infection after vacuum-assisted vaginally delivered infants of asymptomatic mothers. J Perinatol 2004;24(3):147-9.
- James SH, Kimberlin DW. Neonatal herpes simplex virus infection. Infect Dis Clin N Am 2015;29(3):391-400. doi: 10.1016/j.idc.2015.05.001.
- Kimberlin DW, Lin CY, Jacobs RF, et al. Natural history of neonatal herpes simplex virus infections in the acyclovir era. Pediatrics 2001;108(2):223-9.
- Long SS, Pool TE, Vodzak J, Daskalaki I, Gould JM. Herpes simplex virus infection in young infants during 2 decades of empiric acyclovir therapy. Pediatr Infect Dis J 2011;30(7):556-61.
- Adamiak B, Trybala E, Mardberg K, et al. Human antibodies to herpes simplex virus type 1 glycoprotein C are neutralizing and target the heparan sulfate-binding domain. Virology 2010;400(2):197-206.
- Malm G, Berg U, Forsgren M. Neonatal herpes simplex: Clinical findings and outcome in relation to type of maternal infection. Acta Paediatr 1995;84(3):256-60.
- Whitley RJ, Yeager A, Kartus P, et al. Neonatal herpes simplex virus infection: Follow-up of vidarabine therapy. Pediatr 1983;72(6):778-85.
- Kimberlin DW, Jacobs RF, Powell DA, et al. Safety and efficacy of high-dose acyclovir in the management of neonatal herpes simplex virus infections. Pediatr 2001;108(2);230-8.
- Whitley R, Arvin A, Prober C, et al. Predictors of morbidity and mortality in neonates with herpes simplex infections: The National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group. N Engl J Med 1991;324(7):450-4.
- Kimberlin DW, Whitley RJ, Wan W, et al. Oral acyclovir suppression and neurodevelopment after neonatal herpes. N Engl J Med 2011;365(14):1284-92.
- Kimura H, Futamura M, Kito H, et al. Detection of viral DNA in neonatal herpes simplex virus infections: Frequent and prolonged presence in serum and cerebrospinal fluid. J Infect Dis 1991;164(2):289-93.
- Wada K, Mizoguchi S, Ito Y, et al. Multiplex real-time PCR for the simultaneous detection of herpes simplex virus, human herpesvirus 6, and human herpesvirus 7. Microbiol Immunol 2009;53(1):22-9.
- Kimura H, Ito Y, Futamura M, et al. Quantitation of viral load in neonatal herpes simplex virus infection and comparison between type 1 and type 2. J Med Virol 2002;67(3):349-53.
- Tod M, Lokiec F, Bidault R, De Bony F, Petitjean O, Aujard Y. Pharmacokinetics of oral acyclovir in neonates and in infants: A population analysis. Antimicrob Agents Chemother 2001;45(1):150-7.
- Demmler-Harrison GJ. Neonatal herpes simplex virus (HSV) infection: Management and prevention. UpToDate, January 15, 2025. (Accessed November 3, 2025).
- Sanchez PJ, Demmler-Harrison GJ. Viral infections of the fetus and neonate. In: Feigin RD, Cherry JD, eds. Textbook of Pediatric Infectious Diseases, 6th edn Philadelphia: Saunders, 2009:895.
- Public Health Agency of Canada. Routine practices and additional precautions for preventing the transmission of infection in health care settings. (Accessed November 3, 2025).
Disclaimer: The recommendations in this position statement do not indicate an exclusive course of treatment or procedure to be followed. Variations, taking into account individual circumstances, may be appropriate. Internet addresses are current at time of publication.