Practice point
Acute management of croup in the emergency department

Posted: May 24, 2017 | Updated: Mar 6, 2026
Principal author(s)
Oliva Ortiz-Alvarez; Canadian Paediatric Society, Acute Care Committee
Abstract
Croup is one of the most common causes of upper airway obstruction in young children. It is characterized by sudden onset of barky cough, hoarse voice, inspiratory stridor and respiratory distress caused by upper airway inflammation secondary to a viral infection. Published guidelines for the diagnosis and treatment of croup advise using steroids as the mainstay treatment for all children who present to emergency department (ED) with croup symptoms. Dexamethasone, given orally as a single dose at 0.6 mg/kg, is highly efficacious in treating croup symptoms. Despite the evidence supporting the use of steroids as the cornerstone of croup treatment, there is significant practice variation among physicians treating croup in the ED. This practice point discusses evidence-based management of typical croup in the ED.
Keywords: Corticosteroids, Croup, Dexamethasone, Epinephrine, Heliox
BACKGROUND AND EPIDEMIOLOGY
Most children with croup have mild and short-lived symptoms, with <1% of cases experiencing severe symptoms[1][2]. However, croup accounts for significant rates of emergency department (ED) visits and hospitalizations in Canada, with one population-based study in Alberta reporting that 3.2% to 5.1% of all ED visits in children <2 years of age were related to croup[3]. Less than 6% of children presenting to ED with croup symptoms require hospitalization and when they are admitted, it is usually for a short stay[3]. Endotracheal intubation is rare (at 0.4% to 1.4% of hospitalized cases) and death is exceptionally rare (at 0.5% of intubated cases)[4]. There is considerable variation in clinical practice for croup. In small Canadian EDs, children with croup are less likely to receive steroids than in larger centres, while the use of antibiotics and beta-agonists (which are rarely indicated in the care of children with croup) is more frequent than in larger EDs[5][6].
ETIOLOGY AND PATHOPHYSIOLOGY
Croup is caused by viral infections of the respiratory tract and most commonly by parainfluenza types 1 and 3 viruses. Other implicated viruses are influenza A and B, adenovirus, respiratory syncytial virus and metapneumovirus[7]. During the coronavirus disease -19 (COVID 19) pandemic, children infected with the omicron variant of SARS-CoV-2 commonly presented with croup symptoms[8]. These infections cause generalized airway inflammation and edema of the upper airway mucosa. The subglottic region becomes narrowed, causing upper airway obstruction and the symptoms typically associated with croup.
CLINICAL PRESENTATION
Classical croup symptoms have a rapid onset and include barky cough, inspiratory stridor, hoarseness and respiratory distress. Nonspecific symptoms of an upper respiratory illness usually precede the typical croup symptoms, which often worsen at night. Typical croup usually affects children between 6 months and 3 years of age. Symptoms are short-lived, usually lasting 3 to 7 days. In 60% of patients, the barky cough disappears after 48 hours[1]. In <5% of cases, symptoms may last longer than five nights and <5% of children experience more than one episode. In Canada, croup season peaks over the fall and winter[3][9][10].
DIFFERENTIAL DIAGNOSIS
Children who present with croup at <6 months of age or whose symptoms are recurrent, prolonged or unusually severe require further assessment to rule out congenital or acquired airway narrowing[1]. Prolonged duration of croup symptoms associated with fever may be seen with secondary bacterial infection[1]. Less than 1% of children with croup have severe or life-threatening symptoms[1][2], but there are several other life-threatening conditions that may present with stridor. Toxic appearance, drooling and dysphagia are important red flags suggestive of more serious conditions (Table 1).
| Table 1. | |
| Differential diagnosis | |
| Condition | Characteristics |
| Bacterial tracheitis | High fever, toxic appearance and poor response to nebulized epinephrine |
| Retropharyngeal, parapharyngeal, peritonsillar abscesses | High fever, neck pain, sore throat and dysphagia followed by torticollis, drooling, respiratory distress and stridor |
| Epiglottitis | Absence of barky cough, sudden onset of high fever, dysphagia, drooling, toxic appearance, anxious appearance and sitting forward in the ‘sniffing’ position |
| Aspiration or ingestion of a foreign body | Croupy cough, choking episode, wheezing, hoarseness, biphasic stridor, dyspnea and decreased air entry |
| Acute allergic reaction (anaphylaxis or angioneurotic edema) | Rapid onset of dysphagia, wheezing, stridor and possible cutaneous allergic signs, such as urticarial rash |
|
Adapted from Bjornson and Johnson[10] |
|
TREATMENT
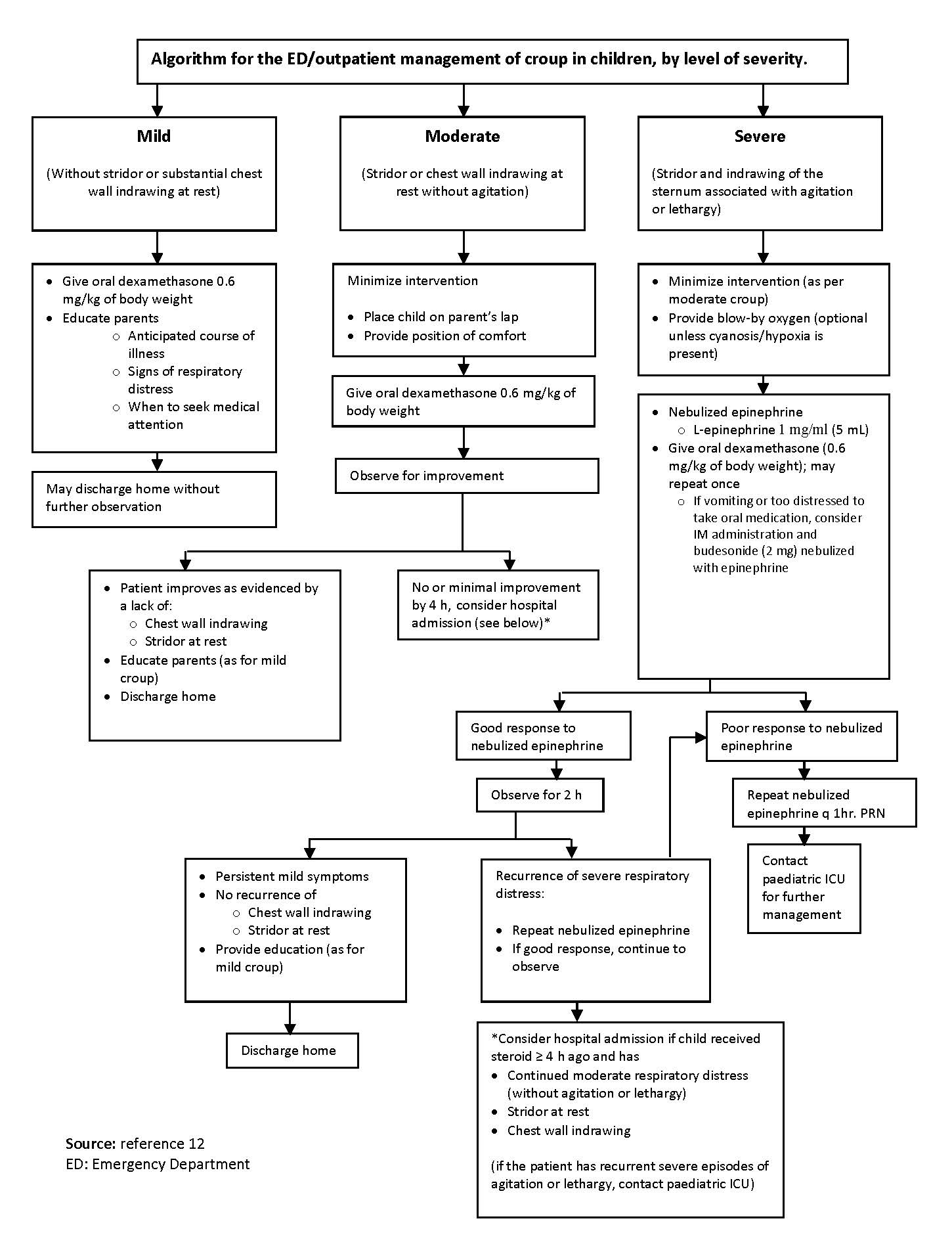
The severity of the child’s respiratory distress on presentation to the ED should guide management (Table 2). Clinical scores used in research studies have not been shown to improve clinical care[11][12]. Most clinicians characterize respiratory distress as mild, moderate, severe or impending respiratory failure. Using this classification, an algorithm for the outpatient management of croup in children was developed through expert consensus[13]. Children presenting with severe distress or impending respiratory failure should be referred to paediatric intensive care or to anaesthesia for advanced care when clinical response to initial treatment is poor or not sustained.
| Table 2. | ||||
| Croup severity | ||||
| Feature | Mild | Moderate | Severe | Impending respiratory failure |
| Barky cough | Occasional | Frequent | Frequent | Often not prominent due to fatigue |
| Stridor | None or minimal at rest | Easily audible at rest | Prominent inspiratory and occasionally expiratory | Audible at rest, but may be quiet or hard to hear |
| In-drawing suprasternal and/or intercostal | None to mild | Visible at rest | Marked or severe | May not be marked |
| Distress, agitation or lethargy (CNS hypoxia) | None | None to limited | Substantial lethargy may be present | Lethargy or decreased level of consciousness |
| Cyanosis | None | None | None | Dusky or cyanotic without supplemental oxygen |
|
CNS Central nervous system. Modified from Bjornson and Johnson[1]. |
||||
Overall, the recommended treatment for croup involves the following measures (Figure 1).
General care
Children should be made comfortable and health care providers must take special care not to frighten them during assessment and treatment. There is no evidence to support the treatment of croup with the use of humidified air[14]. Mist tents separate children from their caregivers, can disperse fungus and therefore are not recommended[14]. The use of antipyretics is beneficial for reducing fever and discomfort.
Corticosteroids
The clinical benefit of corticosteroids in croup is well established[2][15]-[17] and should be considered for treating all children presenting with croup symptoms ranging from mild to severe. Improvement generally begins within 2 to 3 hours after a single oral dose of dexamethasone and persists for 24 to 48 hours[2][16][17]. A 2023 Cochrane review analyzed results from 45 randomized controlled trials (RCTs) (n=5888) associating corticosteroids with greater clinical improvement as measured by improved Westley croup scores at 2 hours; improvement was also noted at 6, 12, and 24 hours[15]. Dexamethasone was the corticosteroid tested in most of these clinical trials. Two studies compared oral dexamethasone with oral prednisolone and found both therapies to be equally effective at 2 and 6 hours[15].
Administering corticosteroids by the oral or intramuscular route is as efficacious or superior to the nebulized form of medication[1][5]. Adding inhaled budesonide to oral dexamethasone was not found to provide extra benefit in children admitted with croup[18]. From a practical perspective, oral dexamethasone is less associated with vomiting[15]. The oral route is preferred. When the child with croup has persistent vomiting or significant respiratory distress, administering corticosteroids by the intramuscular route may be indicated[1]. The dexamethasone dose used in most clinical trials is 0.6 mg/kg/dose[15]. It is unclear from studies using doses of 0.15 mg/kg to 0.3 mg/kg whether these smaller doses are equally effective[19]. One meta-analysis of six studies suggested that a higher dose could be more beneficial in children with severe disease[16].
Overall, children treated with corticosteroids have fewer return visits or admissions to the hospital. Fully one-half of children with mild croup treated with corticosteroids are unlikely to need further medical care for ongoing symptoms. Their sleep is improved and their parents report less stress[2]. In children with moderate to severe croup treated with corticosteroids, there was a reported average reduction of 12 hours in length of stay in the ED or hospital. There was a 10% reduction in the need for treatment with nebulized epinephrine and a 50% reduction in both the number of return visits and in hospitalization rates[15]. There have been no adverse events associated with a single dose of corticosteroids for treatment of croup.
Epinephrine
Nebulized epinephrine is recommended for moderate to severe croup. Reports of administering epinephrine in children with severe croup have demonstrated a lower number of cases requiring intubation or tracheotomy[20]. When compared with a placebo, nebulized epinephrine improved signs of respiratory distress within 10 to 30 minutes of initiating treatment. Clinical effect is sustained for at least 1 hour, but disappears after 2 hours[20]. The first prospective trial assessing safe discharge after treating paediatric outpatients with a combination of dexamethasone and nebulized epinephrine, and including observation for 2 to 4 hours, supported the safety of this measure[21]. There were no adverse outcomes. These results, along with data from two retrospective cohort studies, clearly support the safe discharge of children, providing that symptoms of croup do not recur 2 to 4 hours after treatment[1][22][23].
Traditionally, racemic epinephrine has been used to treat children with croup. Racemic epinephrine is not readily available in Canada. However, one randomized controlled trial demonstrated that nebulized 1:1000 L-epinephrine is safe and equally effective. Equivalent doses of either 0.5 mL racemic epinephrine or 5 mL of 1:1000 L-epinephrine are equally effective. These standard doses can be used in all patients irrespective of their age and weight[24].
Heliox
A heliox or helium-oxygen mixture can reduce respiratory distress in children with severe croup. A possible mechanism of action is that the lower density of helium gas decreases airflow turbulence in a narrowed airway. Heliox is occasionally used in severe cases to avoid intubation. Heliox has not been shown to improve croup symptoms when compared with standard treatments and therefore is not routinely recommended[25].
Other therapies
The use of antibiotics and short-acting beta-2-agonist bronchodilators in children with typical croup are rarely indicated because of the low incidence of bacterial infection (<1:1000 cases of croup)[15] as well as for physiological reasons. An otorhinolaryngology (ORL) consultation for airway evaluation is indicated when croup symptoms are persistently severe despite treatment. Outpatient referral to ORL is recommended for children with multiple croup episodes and for those who present outside the usual age group for typical croup (Figure 1).
|
Algorithm for the outpatient management of crop in children, by level of severity.
|
Acknowledgements
This practice point has been reviewed by the Community Paediatrics and Infectious Diseases and Immunization Committees of the Canadian Paediatric Society, as well as by the CPS Paediatric Emergency Section Executive.
CANADIAN PAEDIATRIC SOCIETY ACUTE CARE COMMITTEE
Members: Carolyn Beck MD, Laurel Chauvin-Kimoff MD (Chair), Isabelle Chevalier MD (Board Representative), Catherine Farrell MD (past member), Jeremy Friedman MD (past member), Kristina Krmpotic MD, Kyle McKenzie MD, Oliva Ortiz-Alvarez MD, Evelyne D. Trottier MD
Liaisons: Dominic Allain MD, CPS Paediatric Emergency Section; Niraj Mistry MD, CPS Hospital Paediatrics Section
Principal author: Oliva Ortiz-Alvarez MD
Updated January 2026: Oliva Ortiz-Alvarez MD
References
- Bjornson CL, Johnson DW. Croup in children. CMAJ 2013;185(15):1317–23.
- Bjornson CL, Klassen TP, Williamson J, et al.; Pediatric Emergency Research Canada Network. A randomized trial of a single dose of oral dexamethasone for mild croup. N Engl J Med 2004;351(13):1306–13.
- Rosychuk RJ, Klassen TP, Metes D, Voaklander DC, Senthilselvan A, Rowe BH. Croup presentations to emergency departments in Alberta, Canada: A large population-based study. Pediatr Pulmonol 2010;45(1):83–91.
- McEniery J, Gillis J, Kilham H, Benjamin B. Review of intubation in severe laryngotracheobronchitis. Pediatrics 1991;87(6):847–53.
- Hampers LC, Faries SG. Practice variation in the emergency management of croup. Pediatrics 2002;109(3):505–8.
- Johnson DW, Craig W, Brant R, Mitton C, Svenson L, Klassen TP. A cluster randomized controlled trial comparing three methods of disseminating practice guidelines for children with croup [ISRCTN73394937]. Implement Sci 2006;(1):10.
- Rihkanen H, Rönkkö E, Nieminen T, et al. Respiratory viruses in laryngeal croup of young children. J Pediatr 2008;152(5):661–5.
- Brewster RCI, Parsons C, Laird-Gion J, et al. COVID-19-associated croup in children. Pediatrics 2022;149(6):e2022056492.
- Rosychuk RJ, Klassen TP, Voaklander DC, Senthilselvan A, Rowe BH. Seasonality patterns in croup presentations to emergency departments in Alberta, Canada: A time series analysis. Pediatr Emerg Care 2011;27(4):256–60.
- Bjornson CL, Johnson DW. Croup in the paediatric emergency department. Paediatr Child Health 2007;12(6):473–7.
- Fitzgerald DA. The assessment and management of croup. Paediatr Respir Rev 2006;7(1):73–81.
- Chan A, Langley J, Leblanc J. Interobserver variability of croup scoring in clinical practice. Paediatr Child Health 2001;6(6):347–51.
- TREKK Croup Development Team (August 2023)(Johnson D, Turnbull J, Eagleson G and Bialy L) Croup:Bottom line recommendations. Translating Emergency Knopwledge for Kids (TREKK) (Accessed January 08,2026).
- Moore M, Little P. Humidified air inhalation for treating croup. Cochrane Database Syst Rev 2006;(3):CD002870.
- Aregbesola A, Tam CM, Kothari A, Le ML, Ragheb M, Klassen TP. Glucocorticoids for croup in children. Cochrane Database Syst Rev. 2023 Jan 10;1(1):CD001955
- Parker CM, Cooper MN. Prednisolone Versus Dexamethasone for Croup: a Randomized Controlled Trial. Pediatrics. 2019 Sep;144(3):e20183772.
- Ausejo M, Saenz A, Pham B, et al. The effectiveness of glucocorticoids in treating croup: Meta-analysis. BMJ 1999;319(7210):595–600.
- Geelhoed GC. Budesonide offers no advantage when added to oral dexamethasone in the treatment of croup. Pediatr Emerg Care 2005;21(6):359–62.
- Geelhoed GC, Macdonald WB. Oral dexamethasone in the treatment of croup: 0.15 mg/kg versus 0.3 mg/kg versus 0.6 mg/kg. Pediatr Pulmonol 1995;20(6):362–8.
- Bjornson C, Russell KF, Vandermeer B, Durec T, Klassen TP, Johnson DW. Nebulized epinephrine for croup in children. Cochrane Database Syst Rev 2013;10:CD006619.
- Prendergast M, Jones JS, Hartman D. Racemic epinephrine in the treatment of laryngotracheitis: Can we identify children for outpatient therapy? Am J Emerg Med 1994;12(6):613–6.
- Kelley PB, Simon JE. Racemic epinephrine use in croup and disposition. Am J Emerg Med 1992;10(3):181–3.
- Corneli HM, Bolte RG. Outpatient use of racemic epinephrine in croup. Am Fam Physician 1992;46(3):683–4.
- Zhang L, Sanguebsche LS. The safety of nebulization with 3 to 5 ml of adrenaline (1:1000) in children: An evidence based review. J Pediatr (Rio J) 2005;81(3):193–7.
- Moraa I, Sturman N, McGuire TM, van Driel ML. Heliox for croup in children. Cochrane Database Syst Rev 2021;8(8):CD006822.
Disclaimer: The recommendations in this position statement do not indicate an exclusive course of treatment or procedure to be followed. Variations, taking into account individual circumstances, may be appropriate. Internet addresses are current at time of publication.